Gait disorder rehabilitation using vision and non-vision based sensors: A systematic review
DOI:
https://doi.org/10.17305/bjbms.2012.2484Keywords:
Gait disorder, rehabilitation, sensor technologyAbstract
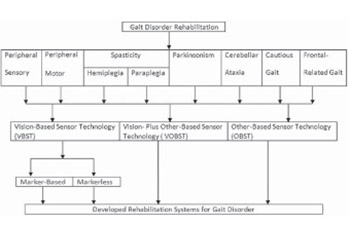
Even though the amount of rehabilitation guidelines has never been greater, uncertainty continues to arise regarding the efficiency and effectiveness of the rehabilitation of gait disorders. This question has been hindered by the lack of information on accurate measurements of gait disorders. Thus, this article reviews the rehabilitation systems for gait disorder using vision and non-vision sensor technologies, as well as the combination of these. All papers published in the English language between 1990 and June, 2012 that had the phrases “gait disorder” “rehabilitation”, “vision sensor”, or “non vision sensor” in the title, abstract, or keywords were identified from the SpringerLink, ELSEVIER, PubMed, and IEEE databases. Some synonyms of these phrases and the logical words “and” “or” and “not” were also used in the article searching procedure. Out of the 91 published articles found, this review identified 84 articles that described the rehabilitation of gait disorders using different types of sensor technologies. This literature set presented strong evidence for the development of rehabilitation systems using a markerless vision-based sensor technology. We therefore believe that the information contained in this review paper will assist the progress of the development of rehabilitation systems for human gait disorders.
Citations
Downloads
Downloads
Additional Files
Published
How to Cite
Accepted 2017-09-22
Published 2012-08-20





