Anatomical variations and morphometric study of the optic strut and the anterior clinoid process
DOI:
https://doi.org/10.17305/bjbms.2012.2502Keywords:
optic strut, anterior clinoid process, caroticoclinoid foramenAbstract
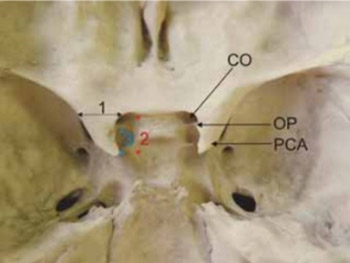
The optic strut and the anterior clinoid process represent bony structures that are closely related to anatomically and clinically significant elements such as the cavernous sinus, the internal carotid artery, the optic nerve and the pituitary gland. The objective of our study was to quantify dimensions of the optic strut and anterior clinoid process, and to determine variations in positions and forms of these structures. A descriptive anatomical study was performed on 200 dry human skulls. We analyzed dimensions and variations in position of the optic strut, dimensions of the anterior clinoid process as well as the incidence and forms of the caroticoclinoid foramen. The average thickness of the optic strut on skulls belonging to males was 3 mm and 2.8 mm on those belonging to females. The optic strut was most commonly attached to the anterior two fifths on the lower side of the anterior clinoid process. On the male skulls the average width of the anterior clinoid process was 9.4 mm (right) and 9.1 mm (left). Its length was 9.9 and 9.3 mm. On female skulls the average width of the process was 8.7 mm (right) and 8.3 mm (left), while the length measured 9.3 mm on the right and 8.9 mm on the opposite side. In our sample, a complete caroticoclinoid foramen appeared in 4.25%, a contact form in 2.75%. At last, an incomplete form of the foramen was observed in 9.75%. The anatomic variations of the investigated structures must be considered during the approaches to the cavernous sinus and neurovascular elements of the sellar region.
Citations
Downloads
Downloads
Additional Files
Published
How to Cite
Accepted 2017-09-26
Published 2012-05-20





