Xanthomas of the stomach: a report of two cases
DOI:
https://doi.org/10.17305/bjbms.2012.2512Keywords:
xanthoma, stomach, differential diagnosi, CD68 antigen, cytokeratin MNF116Abstract
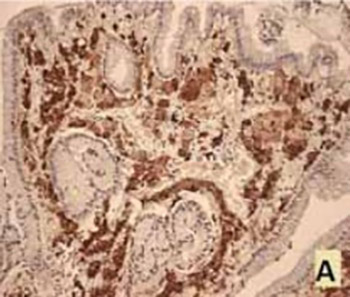
Gastrointestinal tract xanthomas are non tumor, well demarcated mucosal lesions that consist of foamy histiocytes, most commonly diagnosed in the stomach. The histologic appearance of xanthomas can resemble certain malignant lesions. After retrospective data base search, we have encountered only 2 cases of xanthomas, both in the antral part of the stomach. Lamina propria of the mucosa contained rare, chronic inflammatory infiltrate and clusters of oval and polygonal cells with abundant, foamy cytoplasm. The cytoplasm of described cells did not show the presence of mucin (Periodic acid-Schiff (PAS) and Alcian blue staining). The cells showed distinct cytoplasmic CD68 positivity and CKMNF116 negativity, which confirmed the diagnosis of xanthoma. Given the frequent association of xanthomas and known precancerous lesions of gastric mucosa, and occasional coexistence of malignant change, we need to pay attention to its diagnosis, and it is advisable to use both histochemical and immunohistochemical methods.
Citations
Downloads
Downloads
Additional Files
Published
How to Cite
Accepted 2017-09-29
Published 2012-05-20





