Intrauterine blood transfusion in immune hydrops fetalis, corrects middle cerebral artery Doppler velocimetry very quickly
DOI:
https://doi.org/10.17305/bjbms.2012.2532Keywords:
Rh isoimmunization, middle cerebral artery, peak systolic velocimetry, intrauterine transfusionAbstract
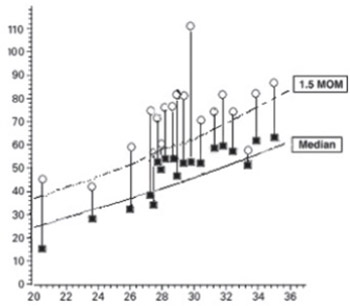
The aim of our study was to evaluate the middle cerebral artery velocimetry before and after intrauterine blood transfusion in immune hydrops fetalis. The current study was conducted in a tertiary research hospital, from February 2009 to January 2011. Nineteen intrauterine blood transfusions performed during the study period. The factors recorded were age of the mothers, gestational weeks, pre-transfusion fetal hematocrit and post-transfusion fetal hematocrit, and also middle cerebral artery peak systolic velocimetry (MCA-PSV) was detected and recorded before and after intrauterine transfusion. A control group of twenty two cases for normal MCA doppler velocimetry was also included to the study. During the study, a total of eleven rhesus isoimmunized pregnancies underwent intrauterine blood transfusions at our perinatal diagnose unit. Before transfusion seventeen severe and two moderate anemias were detected and mean MoM of MCA-PSV was 1.76±0.38 MoM. Post transfusion mean MoM of MCA-PSV in the patient group and control group were 1.08±0.22 MoM and 0.96±0.21 MoM, respectively. The mean MCA-PSV values were higher in RI fetuses than post transfusion and control group. In current study, we found that MCA-PSV is a valuable parameter in detecting fetal anemia requiring intrauterine transfusion and mean MCA-PSV values is higher than 1.5 MoM in fetuses with anemia. And also decrease in MCA-PSV just after transfusion in anemic fetuses showed the quick response of the fetus to correction of anemia.
Citations
Downloads
Downloads
Additional Files
Published
Issue
Section
Categories
How to Cite
Accepted 2017-10-04
Published 2012-02-20





