Local Cellular Immune Response in Dysplastic Epithelial Lesions of the Flat Colonic Mucosa
DOI:
https://doi.org/10.17305/bjbms.1998.3607Keywords:
immunocompetent cells, epithelial dysplasia, immunological techniques, intestinal neoplasiaAbstract
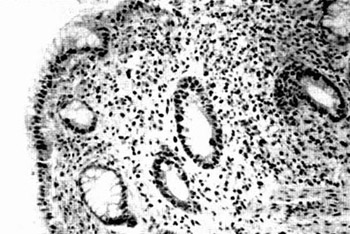
This is an immunohistochemical study of the local cellular immune response characteristic in inflammatory-regenerative and dysplastic flat colonic mucosa. The aim of this study is to determine a possible existence of the mononuclear cellular infiltration specificity which could be important for the prognosis in further development of dysplastic lesion. Biopsy specimens from 170 patients (specimens stained by hematoxylin eosin) were examined. 74 specimens showed inflammatory-regenerative changes and 96 had dysplastic changes (38 with mild dys-plasia, 28 with moderate dysplasia and 30 with severe dysplasia). Three monoclonal antibodies were used for the identification of mononuclear cells in the inflammatory cellular infiltration in the lamina propria of colonic mucosa. The inflammatory cells type and their location in respect of the epithelial cells and lesion itself were analysed and their number was determined by the semi-quantitative method. T lymphocytes were the dominant cells of local immune response in dysplastic lesions while macrophages were less present and B lymphocytes, as rare cells, were present in sporadic cases. It is notified that increase in the extent of dysplasia was followed by increase in the number of macrophages and T lymphocytes in particular. Immediate contact between macrophages and T lymphocytes in epithelial dysplasia was found in a small number of cases and was mostly independent from the intensity of dysplasia. Signs of the direct lytical effect of the mononuclear ceils on dysplastic epithelial cells were not observed in this contact. It seems that epithelial dysplasia does not provoke more significant local immune response which is the most probably a part of the chronic non-specific inflammation that has a negative influence on further development of the lesion. The conclusion is that local immune response in the dysplastic alteration of flat colonic mucosa has no importance in further prognosis of the lesion.
Citations
Downloads
Published
How to Cite
Accepted 2018-05-14
Published 1998-02-20





