The 2019 measles epidemic in Bosnia and Herzegovina: What is wrong with the mandatory vaccination program?
DOI:
https://doi.org/10.17305/bjbms.2019.4266Keywords:
Bosnia and Herzegovina, epidemic, measles, MMR, vaccinationAbstract
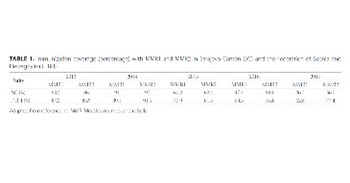
Measles is a highly contagious and communicable viral disease which may be prevented by a sustained vaccination program. Due to missed vaccination, two major epidemics of measles (1997–1999 and 2014–2015) have been recorded after the war in Bosnia and Herzegovina (BH) with over 10,000 patients registered. According to the World Health Organization, BH is categorized as a country with endemic transmission of measles. The last measles epidemic was between 2014 and 2015, with 5,083 documented patients in the Federation of BH. In the first four months of 2019, more than 700 measles cases were registered in the same region. Significant transmission rate has been observed in Sarajevo Canton (SC) with 570 documented measles cases. Out of 570 measles cases in SC, 92.5% were unvaccinated. The most affected were children up to 6 years of age (62.8%), with one documented case of death (7-month old infant). In addition to this report, we discussed key stakeholders and possible circumstances responsible for the epidemic. The measles epidemic is still ongoing.
Citations
Downloads