The role of cytoreductive nephrectomy in renal cell carcinoma patients with liver metastasis
DOI:
https://doi.org/10.17305/bjbms.2020.4896Keywords:
Cytoreductive nephrectomy, renal cell carcinoma, liver metastasisAbstract
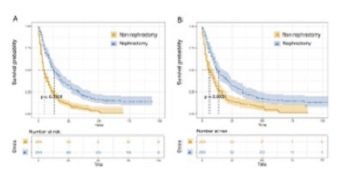
It is widely accepted that renal cell carcinoma (RCC) with liver metastasis (LM) carries a dismal prognosis. We aimed to explore the value of cytoreductive nephrectomy among these patients. Patients were extracted from the Surveillance, Epidemiology, and End Results (SEER) database between 2010 and 2017. The univariate and multivariate Cox proportional hazards models were conducted to select the prognostic predictors of survival. Patients were divided into nephrectomy and non-nephrectomy groups. Propensity score-matching (PSM) analyses were applied to reduce the above factors’ differences between the groups. Overall survival (OS) was compared by Kaplan–Meier analyses. Data from 683 patients were extracted from the database. The univariate Cox regression and multivariate Cox regression revealed that factors including age, histologic type, T and N stages, lung metastasis, brain metastasis, and nephrectomy were significant predictors of survival in the patients. After the PSM analyses, we found that nephrectomy prolonged OS. Nephrectomy can prolong OS in eligible RCC patients with LM.
Citations
Downloads
Downloads
Additional Files
Published
Issue
Section
Categories
How to Cite
Accepted 2020-07-22
Published 2021-04-01





