Morphological aspects of myocardial bridges
DOI:
https://doi.org/10.17305/bjbms.2013.2304Keywords:
human heart, myocardial bridges, morphological aspectsAbstract
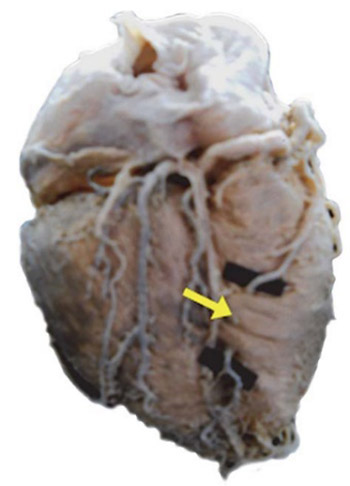
Although some myocardial bridges can be asymptomatic, their presence often causes coronary disease either through direct compression of the “tunnel” segment or through stimulation and accelerated development of atherosclerosis in the segment proximally to the myocardial bridge. The studied material contained 30 human hearts received from the Department of Anatomy. The hearts were preserved 3 to 5 days in 10% formalin solution. Thereafter, the fatty tissue was removed and arterial blood vessels prepared by careful dissection with special reference to the presence of the myocardial bridges. Length and thickness of the bridges were measured by the precise electronic caliper. The angle between the myocardial bridge fibre axis and other axis of the crossed blood vessel was measured by a goniometer. The presence of the bridges was confirmed in 53.33% of the researched material, most frequently (43.33%) above the anterior interventricular branch. The mean length of the bridges was 14.64±9.03 mm and the mean thickness was 1.23±1.32 mm. Myocardial bridge fibres pass over the descending blood vessel at the angle of 10-90 degrees. The results obtained on a limited sample suggest that the muscular index of myocardial bridge is the highest for bridges located on RIA, but that the difference is not significant in relation to bridges located on other branches. The results obtained suggest that bridges located on other branches, not only those on RIA, could have a great contractive power and, consequently, a great compressive force, which would be exerted on the wall of a crossed blood vessel.
Citations
Downloads
Downloads
Additional Files
Published
How to Cite
Accepted 2017-07-23
Published 2013-11-20





