Morphometric measurements of the cranium in congenital bilateral blind males and females
DOI:
https://doi.org/10.17305/bjbms.2013.2331Keywords:
congenital bilateral blind, human, craniometryAbstract
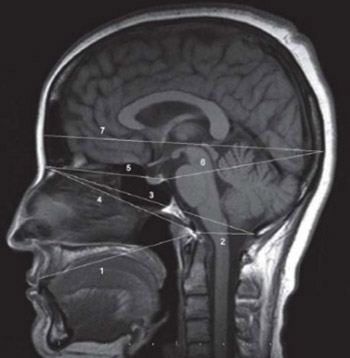
Cranium dimensions differ according to racial, geopraphic, ethnic and nutritional factors. This study will shed light on the question “Is there a difference in the cranial distances measured between congenital bilateral blind people and healthy individuals?” Nine anthropometric measures were performed on the brain MRI midsagittally obtained from male and female congenital bilateral blinds. The anthropometric measures taken included the glabella-opisthocranion, nasion-dorsum sellae, dorsum sellae-opisthocranion, nasion-basion, nasion-opisthion, basion-opisthion, prosthion-basion, basion-vertex and the clival angle. In addition, the supratentorial and infratentorial areas were calculated. Glabella-opisthocranion, nasion-dorsum sellae, nasion-basion, prosthion-basion and clival angle were found to be smaller in the congenital bilateral blind females compared to the healthy group, but these results were not statistically significant. Whereas, other measures out of the basion-opisthion were found to be smaller in the congenital bilateral blind males than in the healthy subjects. Of these results, the distance between glabella-opisthocranion, nasion-dorsum sellae and nasion-basion was significantly smaller compared to the measurements taken from the healthy male group. The infratentorial area was significantly smaller in congenital blind male subjects and the supratentorial area was significantly larger in congenital blind female subjects. This study has revealed that the cranium dimensions of congenital blind people are to different from normal individuals. The most significant difference was in the distance of the nasion-dorsum sellae. The region anterior to the basion and dorsum sellae was prominently smaller. The infratentorial area was significantly smaller in congenital blind male subjects and the supratentorial area was significantly larger in congenital blind female subjects.
Citations
Downloads
Downloads
Additional Files
Published
How to Cite
Accepted 2017-08-07
Published 2013-11-20





