Detrusor contraction duration and strength in the patients with benign prostatic enlargement
DOI:
https://doi.org/10.17305/bjbms.2004.3457Keywords:
BPE, UDM, detrusor contraction durationAbstract
OBJECTIVE: examine detrusor contraction duration (DCD) in relation with obstruction grade and strength of detrusor contractility; analyze individual correlations of this parameter with urodynamic, physiological and symptoms variables in patients with benign prostatic enlargement (BPE).
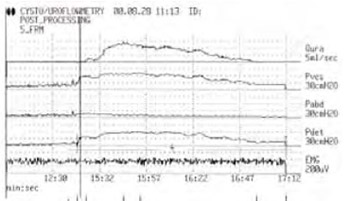
SAMPLE AND METHODOLOGY: 102 patients with proved BPE, underwent complete urodynamic measurements (UDM), namely uroflowmetry, cystometry and pressure/flow studies. Postvoid residual urine (PVR) was measured and the International Prostate Symptom Score (I-PSS) was fulfilled by each patient. Methodology of measurement and definitions of UDM are based on definitions and terminology defined by the International Continence Society.
RESULTS: After grouping the patients (average age 64,7+8,5) related to obstruction grades according to the Schafer nomogram, ANOVA has shown a group extension of the detrusor contraction duration related to higher levels of obstruction (LinPURR 0-VI; p<0,01), which is also followed by stronger detrusor contractility (Pdetmax; p<0,001). Dichotomizing of the patients with DCD cut off point 90 sec. has shown that 67% patients with underactive detrusor have DCD>90 sec, while extension of DCD and increase of the obstruction level are directly related to preserved detrusor contractility only in 20,5% cases. There is neither statistically significant difference of DCD in the patients that are not in obstruction allocated in two groups depending on detrusor contraction strength, (t=1.2, p>0.05); nor in the patients who are in obstruction range, divided on the same way (t=0.568, p>0.05). There is also no difference of the same patients groups regarding PVR (t=1.38 and t=1.17, p>0.05). Individual correlation of DCD with I-PSS has not been shown (r=0.16, p>0.05), although there is a statistically significant correlation with its obstructive subset (r=0.20, p<0.05), as well as, with LinPUR and URA nomograms (r=0.33, r=0.29; respectively, p<0.005) and with Pdetmax (r=0.26, p<0.01), PdetQmax (r=0.24, p<0.05), Qmax and Qaver (r=0.31, p<0.005). DCD does not have individual correlations with patients’ age, prostate volume and with cystometric capacity.
CONCLUSION: DCD is rather independent urodynamical variable, which does not correlate with I-PSS. Generally, DCD is prolonged during obstruction, while extension of DCD only partially depends on detrusor contraction strength. Practically, individual correlations of DCD with the urodynamic factors, which characterize obstructions, are modest.
Citations
Downloads
Downloads
Published
Issue
Section
Categories
How to Cite
Accepted 2018-04-05
Published 2004-02-20





