Braden score at ICU admission predicts 30-day mortality in acute pancreatitis
DOI:
https://doi.org/10.17305/bb.2025.13115Keywords:
Braden score, acute pancreatitis, risk of death, MIMIC-IV databaseAbstract
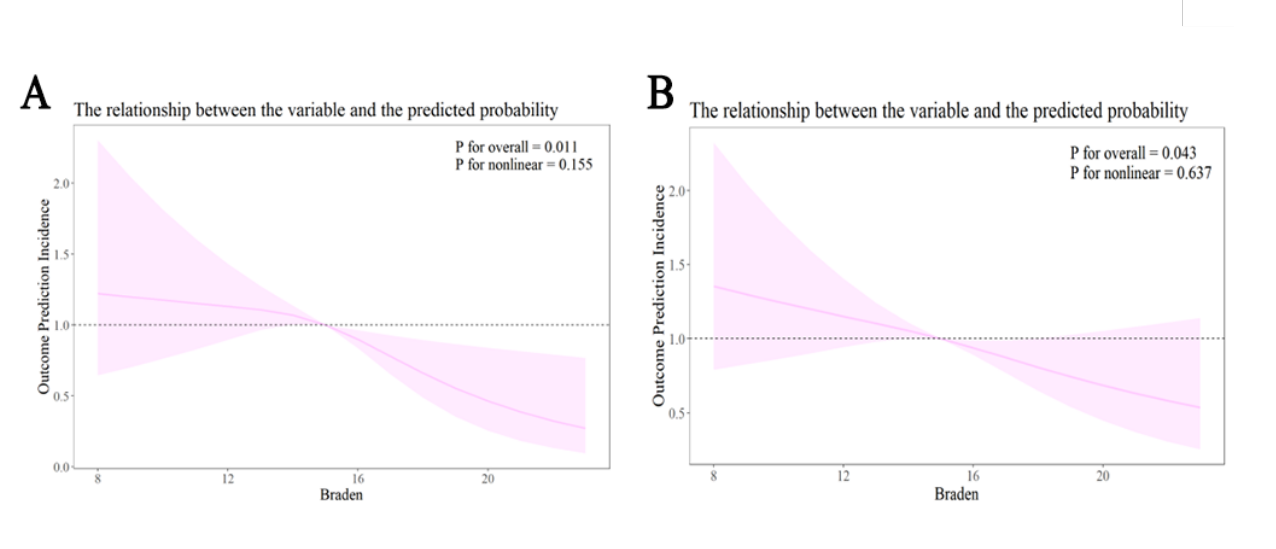
The Braden score, a bedside assessment tool for evaluating the risk of pressure ulcers and frailty, may identify vulnerabilities pertinent to outcomes in acute pancreatitis (AP). However, its prognostic significance in this context remains uncertain. This study aimed to determine whether the Braden score at admission predicts all-cause mortality in intensive care unit (ICU) patients with AP and whether it provides additional value to existing clinical models. In a retrospective single-center cohort study utilizing data from MIMIC-IV v3.1 (2008–2022), we included 1,985 adults diagnosed with AP. We analyzed the Braden score as both a continuous variable and a dichotomous variable (high-risk: ≤15 vs. low-risk: >15), with 30-day mortality as the primary endpoint (with secondary endpoints at 90, 180, and 360 days). Our methodology encompassed Kaplan–Meier analysis, multivariable Cox regression, restricted cubic splines, receiver operating characteristic curves, and calibration assessments. By the 30-day mark, a total of 230 deaths were recorded (11.6%). Each 1-point increase in the Braden score correlated with a 7.7% reduction in mortality risk (HR 0.923, 95% CI 0.873–0.976; p=0.005). Furthermore, patients categorized as low-risk experienced lower mortality rates compared to high-risk patients (HR 0.688, 95% CI 0.501–0.945; p=0.021). The discrimination capability at 30 days was moderate (AUC 0.67, 95% CI 0.63–0.71), with an optimal cutoff score of 15 (sensitivity 61%, specificity 65%) and good calibration; however, performance diminished over longer durations. Incorporating the Braden score into a baseline clinical model enhanced predictive accuracy (AUC 0.712 vs. 0.647; NRI 0.235; IDI 0.040; all p<0.001). The Braden score at ICU admission is independently associated with 30-day mortality in patients with AP, providing moderate, well-calibrated predictions and significant incremental value. This supports its application as an early and straightforward tool for risk stratification, pending prospective validation.
Citations
Downloads
Downloads
Additional Files
Published
Issue
Section
Categories
License
Copyright (c) 2025 Lihong Dong, Hong Wang, Xixiang Yang, Xiaolin Zhu, Chen He

This work is licensed under a Creative Commons Attribution 4.0 International License.





